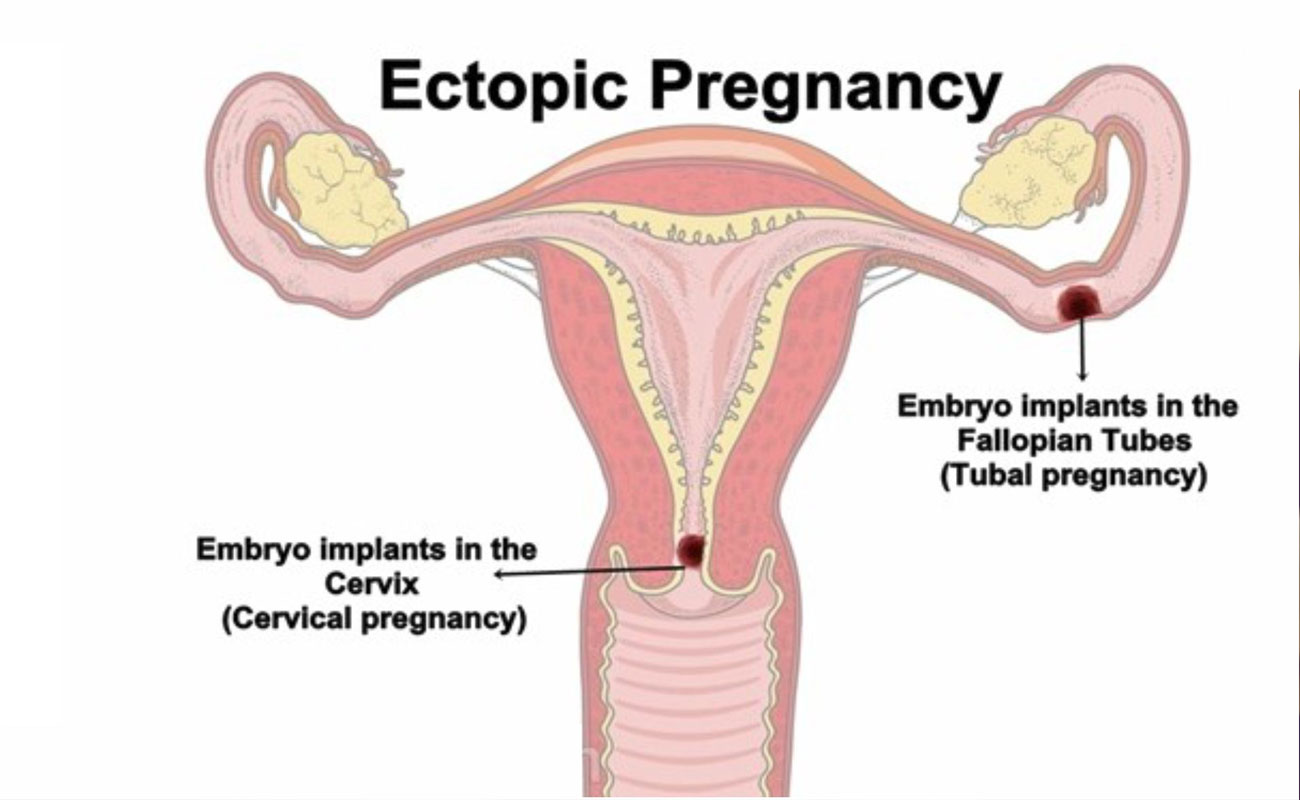
An ectopic pregnancy is when a fertilized egg implants itself outside of the womb, usually in one of the fallopian tubes.

The fallopian tubes are the tubes connecting the ovaries to the womb. If an egg gets stuck in them, it won't develop into a baby and your health may be at risk if the pregnancy continues.
Unfortunately, it's not possible to save the pregnancy. It usually has to be removed using medicine or an operation.
In the UK, around 1 in every 80-90 pregnancies is ectopic. This is around 12,000 pregnancies a year.
All sexually active women are at some risk for an ectopic pregnancy. Risk factors increase with any of the following:
If you have any of the above risk factors, talk to your doctor. You can work with your doctor or a fertility specialist to minimize the risks for future ectopic pregnancies.
Although you may experience typical signs and symptoms of pregnancy, the following symptoms may be used to help recognize a potential ectopic pregnancy:
It is important to contact your doctor immediately if you are experiencing sharp pain that lasts more than a few minutes or if you have bleeding.
An ectopic pregnancy is often caused by damage to the fallopian tubes. A fertilized egg may have trouble passing through a damaged tube, causing the egg to implant and grow in the tube.
Things that make you more likely to have fallopian tube damage and an ectopic pregnancy include:
Some medical treatments can increase your risk of ectopic pregnancy. These include:
If you suspect you may have an ectopic pregnancy, see your doctor immediately. Ectopic pregnancies can’t be diagnosed from a physical exam. However, your doctor may still perform one to rule out other factors.
Another step to diagnosis is a transvaginal ultrasound. This involves inserting a special wand-like instrument into your vagina so that your doctor can see if a gestational sac is in the uterus.
Your doctor may also use a blood test to determine your levels of hCG and progesterone. These are hormones that are present during pregnancy. If these hormone levels start to decrease or stay the same over the course of a few days and a gestational sac isn’t present in an ultrasound, the pregnancy is likely ectopic.
If you’re having severe symptoms, such as significant pain or bleeding, there may not be enough time to complete all these steps. The fallopian tube could rupture in extreme cases, causing severe internal bleeding. Your doctor will then perform an emergency surgery to provide immediate treatment.

Unfortunately, the baby cannot be saved in an ectopic pregnancy. Treatment is usually needed to remove the pregnancy before it grows too large.
The main treatment options are:
These options each have advantages and disadvantages that your doctor will discuss with you.
They'll recommend what they think is the most suitable option for you, depending on factors such as your symptoms, the size of the pregnancy and the level of pregnancy hormone (human chorionic gonadotropin or hCG) in your blood.
If you have no symptoms or mild symptoms and the pregnancy is very small or can't be found, you may only need to be closely monitored, because there's a good chance the pregnancy will dissolve by itself.
This is known as expectant management and the following is likely to happen:
The main advantage of monitoring is that you won't experience any side effects of treatment. A disadvantage is that there's still a small risk of your fallopian tubes splitting open (rupturing) and you may eventually need treatment.

If an ectopic pregnancy is diagnosed early but active monitoring isn't suitable, treatment with a medicine called methotrexate may be recommended.
This works by stopping the pregnancy from growing and is given as a single injection into your buttocks.
You won't need to stay in hospital after treatment, but regular blood tests will be carried out to check if the treatment is working. A second dose is sometimes needed and surgery (see below) may be necessary if it doesn't work.
You need to use reliable contraception for at least three months after treatment, because methotrexate can be harmful for a baby if you become pregnant during this time.
It's also important to avoid alcohol until you're told it's safe, as drinking soon after receiving a dose of methotrexate can damage your liver.
Other side effects of methotrexate include:
There's also a chance of your fallopian tubes rupturing after treatment. You'll be told what to look out for and what to do if you think this has happened.
In most cases, keyhole surgery (laparoscopy) will be carried out to remove the pregnancy before it becomes too large.
During a laparoscopy:
Removing the affected fallopian tube is the most effective treatment and isn't thought to reduce your chances of becoming pregnant again. Your doctor will discuss this with you beforehand and you'll be asked whether you consent to having the tube removed.
Most women can leave hospital a few days after surgery, although it can take four to six weeks to fully recover.
If your fallopian tube has already ruptured, you'll need emergency surgery. The surgeon will make a larger incision in your tummy (laparotomy) to stop the bleeding and repair your fallopian tube, if that is possible.
After either type of surgery, a treatment called anti-D rhesus prophylaxis will be given if your blood type is RhD negative (see blood groups for more information). This involves an injection of a medicine that helps to prevent rhesus disease in future pregnancies.
nhs.uk, healthline.com, webmd.com, nhs.uk, americanpregnancy.org, verywell.com

Submit Comment